Pseudoendocrine sarcoma: rare new entity with unique radiologic and pathologic characteristics.
Pseudoendocrine sarcoma is a rare, recently described intermediate grade sarcoma of uncertain phenotype that most commonly affects the paraspinal location in older patients with a distinctive endocrine/paraganglioma-like morphology and unique CTNNB1 point mutation. While these tumors appear as epithelial or even benign endocrine tumors, these lack markers for such and are highlighted by nuclear expression of beta-catenin.
Zachary Corey et al reported a rare case report; An 82-year-old female presented to an outside health center with a painful right chest wall mass. A subsequent chest radiograph and ultrasound-guided core needle biopsy were performed. Pathologic diagnosis was initially unclear, as this new sarcoma entity is rare and newly described and can mimic a benign or metastatic epithelial or endocrine tumor. This patient’s biopsy and imaging studies were sent to authors’ institution for consultation. AP chest radiograph revealed a subtle right upper chest wall soft tissue density mass without osseous destruction and therefore was difficult to discern. Following the vague suggestion of a mass and corresponding soft tissue density noted on chest radiograph, an ultrasound-guided core needle biopsy was performed. The preprocedural ultrasound revealed an oval, well-circumscribed, homogeneous hypoechoic intramuscular mass. No internal calcification or cystic components were identified. Internal vascularity was observed within the mass on color Doppler imaging with possible feeding vascular pedicles, a subtle clue to diagnosis, in addition to the circumscription and location and presentation, requiring pathology and molecular to confirm the final diagnosis.
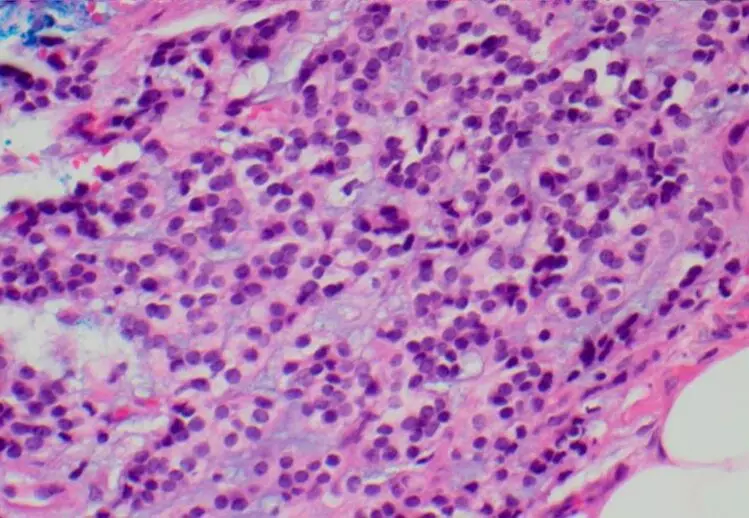
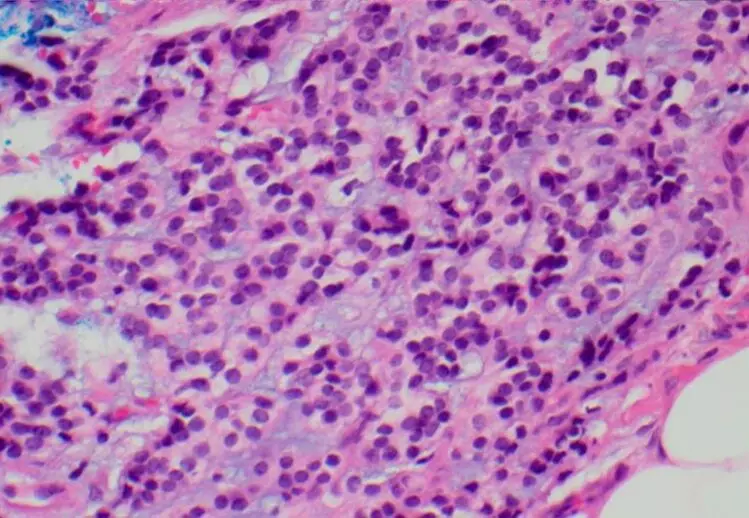
The histopathologic features of this small 3-cm mass reveal a lobular, well delineated, and circumscribed ovoid-shaped tumor with a pseudocapsule. There was a combination of pseudoendocrine/paraganglioma-like features with peripheral capillary vessels, creating the zellballen pattern, admixed with a trabecular (also pseudoendocrine/paraganglioma-like) appearance composed of round to ovoid cells with well-dispersed chromatin and distinctive cytoplasmic borders. The cells demonstrated focal clear cell to cytoplasmic vacuole-appearing features within myxoid stroma that lacked the zellballen pattern, without extracellular psammomatous calcifcations, hyaline globules, metaplastic bone, or necrosis. Mitoses were not significantly increased, and there were no atypical mitoses. Immunostaining was initially ordered by the original pathologist and was positive for nonspecific CD10 and CD99, with mild to focally moderate MIB-1 (indicating intermediate grade sarcoma) and negative for keratin, EMA, MUC4, synaptophysin, chromogranin, and S100 protein (no sustentacular cells), CD34, SMA, desmin, CD68, CD138, CD117, DOG1, GATA-3, CAIX, MITF, Melan-A, and TFE3, excluding endocrine tumors such as benign paraganglioma or malignant adrenal cortical carcinoma and epithelial and melanocytic tumors. A comprehensive sarcoma NGS fusion panel that included BCOR, FUS (SEF), GLI1, NOTCH1/2, PHF1, and STAT6 was negative, failing to reveal a specific diagnosis. The case was sent in consultation and during consultative workup, a nuclear beta-catenin was ordered to exclude this new entity and was positive and a desmoid hotspot panel revealed a unique somatic point mutation for CTNNB1 (c98C>G, p.Ser33Cys in exon 2, hotspot point mutation S33C), supporting the diagnosis of pseudoendocrine sarcoma, the second only of these tumors to exhibit this exact hotspot point mutation. Based on the clinicoradiologic, morphologic, and phenotypic features with CTNNB1 hotspot mutation, a final diagnosis of pseudoendocrine sarcoma was rendered. The patient was treated by complete excision of the mass. Follow-up of more than 4 years demonstrated no evidence for local recurrence or metastasis.
The authors commented – “In summary, this is the twenty-sixth case of newly described pseudoendocrine sarcoma in the chest wall/soft tissue of an elderly woman, diagnosed by having a benign endocrine-like appearance with a complete workup that excluded other entities. The distinctive clinical features, morphologic and phenotypic features with negative markers-favored an intermediate grade sarcoma that was originally negative for a complete sequencing workup. However, the final recognition of this rare novel entity was by a combination of observations by surgeons, radiologists, and pathologists to recognize this rare entity and obtain the final positive nuclear beta-catenin and distinctive CTNNB1 point mutation. Important are the unique features of the current case and the radiologic vascularity that corresponds to microscopic pathologic (Zellballen) vascular features, which resulted in proper diagnosis and management of this potentially metastasizing intermediate grade sarcoma.”
Further reading:
Pseudoendocrine sarcoma: a rare new entity with unique radiologic and pathologic/molecular characteristics
Zachary Corey et al Skeletal Radiology

