Post hoc Analysis: Use of Bisoprolol in NOCAD
Bisoprolol is clinically feasible
option in reducing resting heart rate (RHR) and improving left ventricular
ejection fraction (LVEF), thereby enhancing cardiac function. A recent post-hoc
analysis of the BISOCARD study highlighted these benefits in Indian patients
with non-obstructive coronary artery disease (NOCAD) who had undergone
percutaneous coronary intervention (PCI).
This analysis
provides real-world evidence of bisoprolol’s safety and effectiveness in the
management of patients diagnosed with NOCAD who underwent PCI.
Bisoprolol is a selective β1-receptor antagonist, which
has shown to offer anti-ischemic and anti-hypertensive benefits by reducing
myocardial oxygen demand, lowering RHR, and improving LVEF.
The study has been published in the December 2024 issue of
Cureus.
CAD, NOCAD & Implications
in India:
Indians have the highest rates of CAD, with 20-50% higher
mortality. NOCAD, defined as <50% stenosis in the left main coronary artery,
affects ~50% of patients undergoing elective coronary angiography. Despite
nonobstructive arteries, these patients face recurrent chest pain, reduced
quality of life, and increased risks of mortality and MI, highlighting the need
for proactive care.
Study Overview:
The study was a multi-centered, concurrent, observational, single-arm,
open-label clinical investigation aimed at evaluating bisoprolol’s efficacy and
safety in real-world NOCAD scenarios.
It enrolled 800 CAD patients as
the intent-to-treat (ITT) population across 80 outpatient centers in India,
ensuring broad representation. Among ITT patients, 611 (76.37%) were male and
189 (23.63%) were female, with hypertension present in 100% of cases. The NOCAD
group, representing 47.25% of the ITT population (per-protocol set), consisted
of 378 patients, with 286 (75.66%) males and 92 (24.34%) females. The mean age
of NOCAD patients was 58.63 years, with hypertension, dyslipidemia, and type 2 diabetes
as common risk factors and comorbidities.
The study spanned 24 weeks,
evaluating parameters such as resting heart rate (RHR), systolic blood pressure
(SBP), diastolic blood pressure (DBP), and left ventricular ejection fraction
(LVEF).
Patients received bisoprolol in
doses of 2.5mg, 5mg, and 10mg
per day as per the direction of the physician, and outcomes were assessed at
baseline and after 24 weeks of treatment.
The primary objectives of the
study were to evaluate the change in mean values of RHR and LVEF after 24 weeks
of treatment with bisoprolol. The secondary objectives included assessing
changes in SBP and DBP after 24 weeks and monitoring the occurrence of
treatment-emergent adverse events (TEAEs).
Some of the key findings
from the study are:
Efficacy of Bisoprolol on
Heart Rate, Blood Pressure, and LV Function
Among NOCAD Patients (n=378)
- RHR: Initial RHR in NOCAD patients was 88.3 bpm.
After 24 weeks, it was significantly reduced to 76.15 bpm, showing a change of
-12.14 bpm (p<0.01). - After
24 weeks baseline systolic blood pressure (SBP) of 146.06 mmHg decreased to
129.67 mmHg, showing a reduction of -16.30 mmHg (p<0.01). Similarly, the
diastolic blood pressure (DBP) dropped from a baseline of 91.96 mmHg to 82.92
mmHg, a reduction of -9.05 mmHg (p<0.01) - LVEF: The baseline LVEF was 46.85%. It showed
significant improvement and reached 51.53% at 24 weeks, a change of 4.68%
(p<0.01).
Efficacy in NOCAD Patients in Relation to History of
Ischemic Events
- Among the NOCAD group, 236 patients (62.43%) had
a prior history of ischemic events at baseline. - After 24 weeks of treatment, significant
improvements were observed, including a mean reduction in RHR by 12.46 bpm, SBP
by 19.91 mmHg, DBP by 9.85 mmHg, and a mean increase in LVEF by 5.66%.
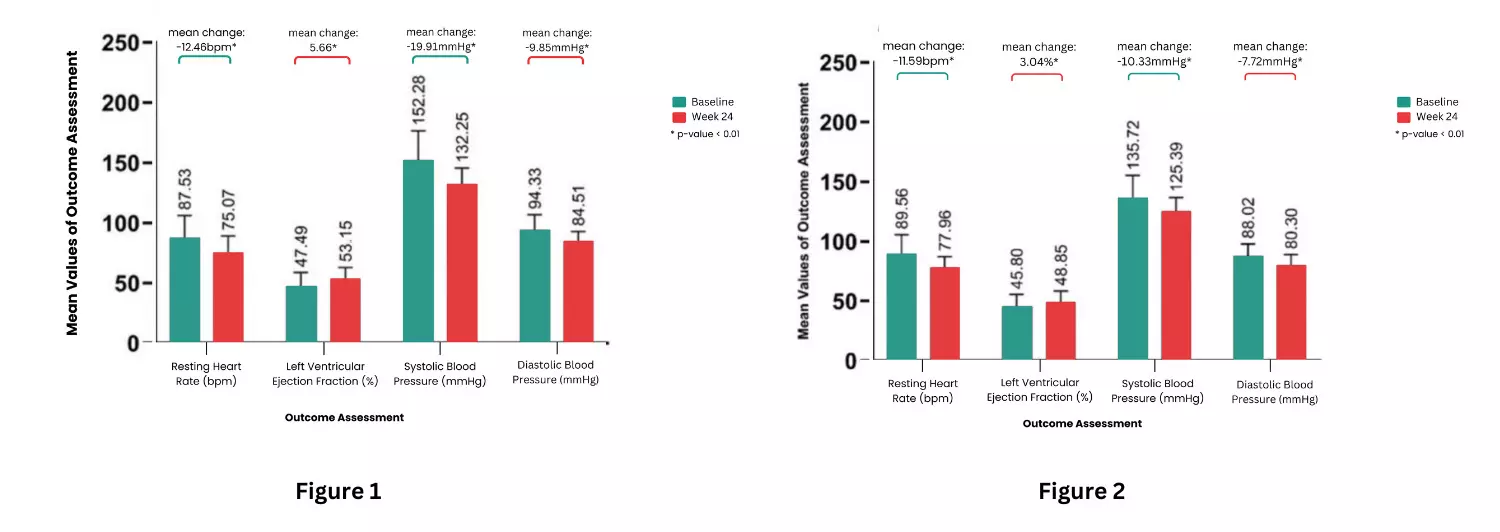
Figure 1: Improvement in Resting Heart Rate, Systolic Blood Pressure, Diastolic Blood Pressure and Left Ventricular Ejection Fraction in Cases with Prior History of Ischemic Events (n = 236)
Figure 2: Improvement in Resting Heart Rate, Systolic Blood Pressure, Diastolic Blood Pressure and Left Ventricular Ejection Fraction in Cases Without Prior History of Ischemic Events (n = 142)
- In the 142 patients (37.57%) without a history
of ischemic events, notable changes included a mean reduction in RHR by 11.59
bpm, SBP by 10.33 mmHg, DBP by 7.72 mmHg, and a mean improvement in LVEF by
3.04%.
Evaluating the Safety of Bisoprolol
Over the 24-week evaluation
period, treatment-emergent adverse events (TEAE) occurred in 60 NOCAD patients
(15.87%), including chest congestion (6.61%), asthenia (5.03%), hypotension
(4.76%), muscular weakness (3.70%), and bradycardia (1.85%). All events were
mild, transient, and did not necessitate treatment withdrawal.
This study found that bisoprolol
was effective and well-tolerated in preserving and improving cardiac function
and parameters, including RHR, SBP, DBP, and LVEF among NOCAD patients in the Indian population with
coexisting hypertension. These findings suggest that adding bisoprolol to
standard NOCAD treatment regimens may improve the quality of care.
*CAD: Coronary Artery Disease; DBP: Diastolic Blood Pressure;
LVEF: Left Ventricular Ejection Fraction, RHR: Resting Heart Rate; SBP: Systolic
Blood Pressure, TEAE: treatment-emergent adverse events
Reference:
1) Pinto
B, Kulkarni GR, Kumar S, Deb A, Fischer L, Khandelwal A, Korukonda KR, Nair R.
Cross-Sectional Analyses to Assess the Clinical Safety and Effectiveness of
Bisoprolol in Patients With Non-obstructive Coronary Artery Disease Who
Underwent Percutaneous Coronary Intervention: A Post-hoc Analysis. Cureus. 2024
Dec 3;16(12):e75021. doi: 10.7759/cureus.75021. PMID: 39749095; PMCID:
PMC11694328.