Simple test can predict risk of heart disease better than current standard
For almost 60 years, measuring cholesterol levels in the blood has been the best way to identify individuals at high risk of cardiovascular disease.
Powered by WPeMatico
Powered by WPeMatico
Powered by WPeMatico
Powered by WPeMatico
Powered by WPeMatico
Powered by WPeMatico

New Delhi- The National Board of Examinations in Medical Sciences (NBEMS) is going to release the application form for the Foreign Medical Graduate Examination (FMGE) June for the academic year 2025 at 3 PM today. The FMGE June 2025 application form will be released on the official website of NBEMS, therefore, interested candidates can fill out the form from registering at the NBE website.
According to the official notice issued by the NBEMS in this regard, the FMGE June 2025 application form will be available on the official website of NBEMS from 03:00 PM today, i.e. 28 April 2025, to 11:55 PM on 17 May 2025. Along with this, the FMGE June 2025 Information Bulletin will also be made available to the candidates from today.
The information bulletin will contain important details for the candidates regarding FMGE June 2025, like eligibility criteria, fee, documents, exam scheme, application process etc.
STEPS TO FILL OUT THE FMGE APPLICATION FORM 2025
STEP 1- Visit the official NBE website.
STEP 2- Register with a valid email ID and mobile number.
STEP 3- Fill out the application form with personal, academic, and contact details.
STEP 4- Upload required documents such as a passport-size photograph, signature, and degree certificates.
STEP 5- Pay the application fee online.
STEP 6- Submit the application form and take a printout for future reference.
NBEMS is going to conduct the FMGE on 26th July 2025 on a computer-based platform at various examination centres across the country. Results are expected by 26th August 2025.
The Foreign Medical Graduate Examination (FMGE), also known as the Screening Test for Foreign Medical Graduates, is a mandatory licensure exam introduced under the Screening Test Regulations, 2002. It is required for Indian citizens or Overseas Citizens of India who have obtained their primary medical qualification from a medical institution outside India and wish to secure provisional or permanent registration with the National Medical Commission (NMC) or any State Medical Council after 15 March 2002. Conducted by the National Board of Examinations in Medical Sciences (NBEMS), the exam ensures that foreign-trained medical graduates meet the standards for practicing medicine in India. Only candidates with a recognized foreign medical qualification (confirmed by the Indian embassy), a provisional pass certificate or degree, and an eligibility certificate (if applicable) are eligible to appear. Upon qualifying, candidates are issued a Screening Test Pass Certificate by NBEMS following biometric and document verification.
To view the notice, click the link below
Powered by WPeMatico

New Delhi: As a precautionary measure following several alleged irregularities, including paper leak in last year’s MBBS entrance test, the National Testing Agency (NTA) has recently announced a dedicated platform to report suspicious claims regarding the NEET 2025. The agency has also advised candidates not to be misled by unscrupulous elements who deceive the NEET 2025 candidates with false claims.
“A dedicated platform has been launched by the National Testing Agency (NTA) to report suspicious claims regarding the NEET(UG) 2025 Examination. NTA advises candidates not to be misled by unscrupulous elements who indulge in malpractice and try to deceive candidates with false claims,” stated the NTA notice regarding reporting of suspicious claims.
Also Read:NEET 2025: NTA notifies Advance Intimation of Exam City for candidates
“Candidates can report any suspicious activities falling in three categories — unauthorised websites or social media accounts claiming access to NEET question paper; individuals claiming access to exam content and impersonators posing as NTA or government officials,” NTA Director General Pradeep Singh Kharola said.
“The reporting form is simple and allows users to describe what they observed, where and when it occurred and upload supporting file. The initiative aligns with the Public Examinations (Prevention of Unfair Means) Act, 2024 which aims to eliminate unfair practices in public examinations and protect the future of aspirants,” he said. The Act contains stringent provisions for offences committed under the Act.
If you witness or suspect any of the above, please report it immediately at the NTA’s website. Reporting of suspicious claims is open until 5:00 PM 1ST on May 4, 2025.
The National Testing Agency (NTA) is conducting the National Eligibility and Entrance Test-Undergraduate (NEET UG) for the academic year 2025 at different locations throughout the country (552 Cities) and abroad (14 Cities) on 04 May 2025 (Sunday) from 02:00 P.M. to 05:00 P.M. in Pen and Paper mode.
The advanced Intimation of Examination City has been released on the NTA website; candidates can check/download their Examination City Intimation slip for NEET UG 2025 using the login credentials.
The Candidates must note that Examination City Intimation slip is not the Admit Card for NEET UG 2025. This is advance information for the allotment of the City where the Examination Centre will be located, to facilitate the candidates. The Admit Card of NEET (UG) 2025 shall be issued later, the notice informed.
STEPS TO DOWNLOAD NEET CITY INTIMATION SLIP
STEP 1- Visit the official website of NTA.
STEP 2- Search for the ‘Download NEET UG 2025 City Intimation Slip’ tab from the candidate activity section.
STEP 3- Enter your NEET 2025 credentials, i.e. application number and date of birth, or password.
STEP 4- Download the NEET 2025 city allotment slip and save it for future reference.
The allotment slip of the NEET-UG 2025 is an important document that mentions the exam city of the candidates. However, the NEET 2025 exam city intimation slip or advanced intimation city slip only contains the name of the exam city.
Candidates willing to appear for the said exam can download the admit card from the NTA website from May 01, 2025. The result is expected to be declared by June 14, 2025.
To view the notice, click on the link below
Powered by WPeMatico

Vijayawada: Renowned cardiologist Dr Pulala Chandrasekhar has been appointed as the new Vice Chancellor of Dr. NTR University of Health Sciences. He has 38 years of experience in different positions in the public healthcare system.
His appointment was confirmed through an order issued by M.T. Krishna Babu, the health special chief secretary. He has been appointed to the position for a term of three years.
Sri Satya Kumar Yadav, the Minister of Health, Family Welfare & Medical Education, called Dr. Chandrasekhar to inform him of his appointment and congratulated him for his remarkable journey from a Medical Officer at a PHC to the position of Vice Chancellor, attributing his success to his hard work, dedication, and outstanding contributions as a cardiologist, teacher and administrator.
Also read- IAS Dr Raghav Langer appointed Secretary of National Medical Commission
Born in August 1960, Dr Chandrasekhar started his career as Civil Assistant Surgeon (Medical Officer) at Primary Health Centre at Sri Rangaraja Puram in Chittor district in 1987 before becoming Assistant Professor at Sri Venkateswara Medical College, Tirupati in 1988, where he worked for about 7 years.
He was then transferred to Government Medical College (GMC), Kurnool. The golden era of the department started in 2003, when Dr. P. Chandrasekhar M.D D.M., took over the charge as HOD of the department of cardiology. From there, he retired in 2023 and was re-employed till his elevation as Vice Chancellor.
Dr. Chandrasekhar worked as Associate Professor, Professor, Superintendent of Government General Hospital, Kurnool, Dean and Principal of GMC, Kurnool. He was in the rank of Additional Director of Medical Education for about four years.
In the process, he acquired rich experience in providing cardiac care, teaching and administration. Born at Pyalakurthi village of Kodumur mandal in Kurnool district, Dr. Chandrasekhar did his MBBS and MD from Kunool Medical College and DM from Christian Medical College, Vellore.
He has several books and publications on various aspects of the functioning of the heart, meant to create awareness among people. He is a Member of various leading national associations of cardiologists.
Dr.Chandrasekhar was awarded a ‘Certificate of Commitment’ by the World Book of Records, London, reports PYNR.
Minister of Health, Family Welfare & Medical Education Sri Satya Kumar Yadav called up Dr.Chandrasekhar, informing him of his appointment and complimenting him for his rise from being a Medical Officer in a PHC to the position of Vice Chancellor through hard work, dedication and distinguished contributions as a cardiologist, teacher and administrator.
Powered by WPeMatico
CVD Risk in Women After 40: Cardiovascular disease (CVD) is the leading cause of death in individuals with type 2 diabetes (T2D) and hypertension. (1) Women in the menopausal transition phase (aged 40–50) are particularly vulnerable yet often underrepresented in preventive care strategies. This transitional period is marked by significant hormonal fluctuations that amplify cardiovascular risk, making primary prevention critically important. (2)
In India, the National Family Health Survey (NFHS)-4 and 5 report that diabetes prevalence among women peaks at 7.8% in the 45–49 age group, with hypertension affecting 31.2% in the same group. Data show that women with diabetes face a 50% higher risk of fatal CVD events compared to men with diabetes (Relative Risk: 3.50 [2.0–4.53] vs. 2.06 [1.81–2.34]). Despite this heightened risk, they are frequently undertreated and inadequately targeted in cardiovascular prevention programs. (2)
Role of Aspirin in Primary Prevention of ASCVD in Diabetes and Hypertension: Diabetes promotes exaggerated platelet activation and aggregation, largely driven by hyperglycemia-induced oxidative stress and inflammation. This is compounded by insulin resistance, which increases intracellular calcium and further enhances platelet activity. As endothelial function deteriorates and lipid-rich plaques become vulnerable to rupture, the overall cardiovascular risk escalates. Aspirin offers cardioprotective benefits in this setting by irreversibly inhibiting COX-1, thereby reducing thromboxane A2 production and platelet aggregation. (3)
The following diagram illustrates shared risk pathways leading to cardiovascular disease in patients with diabetes and hypertension.
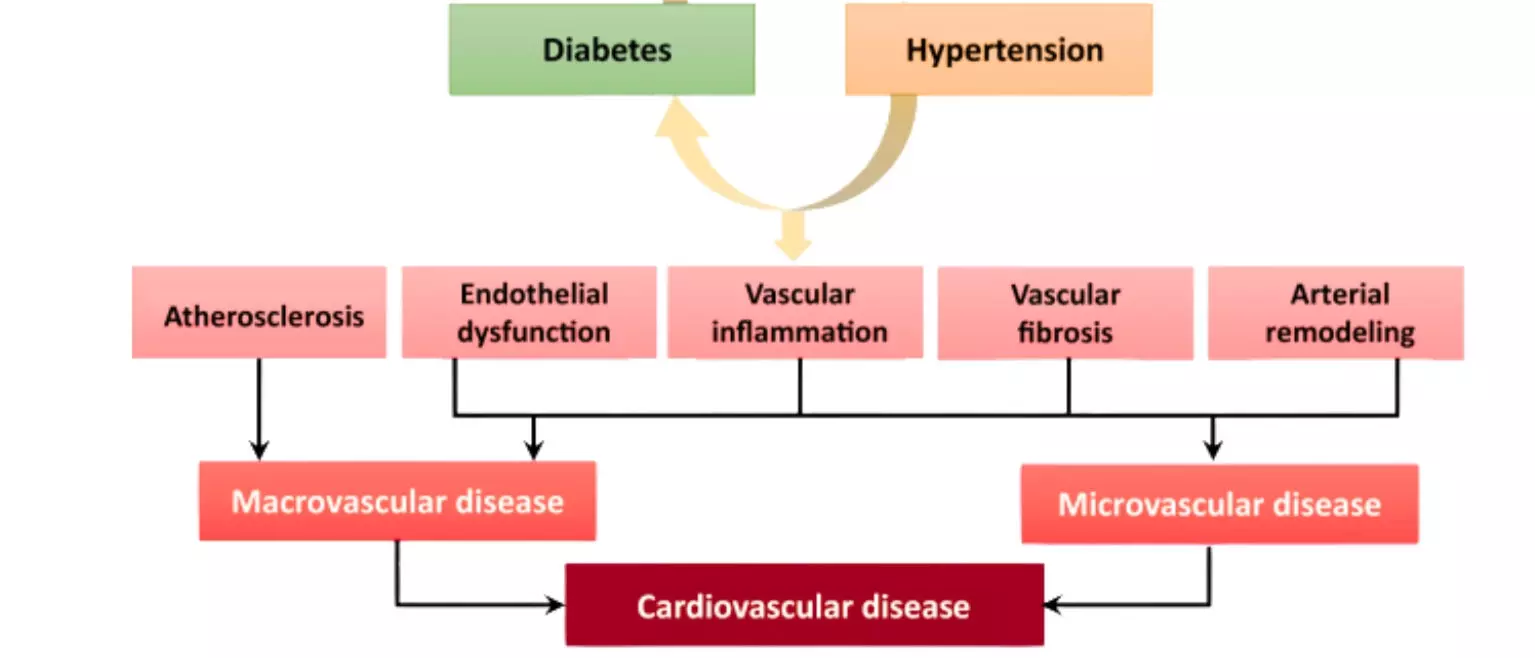
Figure: Pathophysiological Link Between Common Risk Factors- T2D, HT & CVD. Adapted from Petrie JR et al. Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms. Can J Cardiol. 2018;34(5):575–584. doi:10.1016/j.cjca.2017.12.005
Aspirin in Primary Prevention- Women’s Health Study: Women’s Health Study which included 39,876 women aged ≥45 years without prior cardiovascular disease, demonstrated a 17% reduction in total stroke risk with alternate-day low-dose aspirin (100 mg) over 10 years. These findings support a selective approach to aspirin use in women aged ≥45 with elevated CVD risk. (4)
Aspirin in CV Prevention- Review of Guidelines: Accordingly, the 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease also suggests considering low-dose aspirin (75–100 mg/day) for primary prevention in adults aged 40–70 years who are at high ASCVD risk but not at increased risk of bleeding. (5) Similarly, the DCRM 2.0 (Diabetes, Cardiorenal, and Metabolic Diseases Multispecialty Practice Recommendations) Multispecialty Task Force (2024) supports aspirin use (75–100 mg daily) for primary prevention in individuals with at least two major risk factors, such as elevated lipoprotein(a), T2D, hypertension, a family history of premature coronary artery disease, or a coronary artery calcium (CAC) score >100. (6)
Implementation to Clinical Practice–Brief Case Profile: To illustrate practical application, consider a 48-year-old Indian woman undergoing menopausal transition with a history of T2D and hypertension. Her lab values show elevated LDL-C (145 mg/dL), low HDL-C (38 mg/dL), and a high lipoprotein(a) level (55 mg/dL)—a recognized risk factor especially prevalent in South Asian populations.
Given her multiple major cardiovascular risk factors, she would be an appropriate candidate for low-dose aspirin therapy (75–100 mg/day) for primary prevention—provided a structured bleeding risk assessment is conducted. Tools like the Aspirin-Guide app can assist clinicians in individualized decision-making regarding aspirin initiation.
Conclusion: Women aged 40–50 years undergoing menopausal transition and living with type 2 diabetes and hypertension face a significantly heightened risk of cardiovascular disease, particularly in the Indian context where additional risk factors like elevated lipoprotein(a) and abnormal waist-hip ratio are common. Despite this, they remain underrepresented in preventive strategies. Low-dose aspirin therapy, when guided by current recommendations and individualized risk assessments, offers a valuable primary prevention tool to reduce cardiovascular events in this high-risk group.
References:
1. Petrie JR, Guzik TJ, Touyz RM. Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms. Can J Cardiol. 2018;34(5):575-584. doi:10.1016/j.cjca.2017.12.005
2. Huxley R, Barzi F, Woodward M. Excess risk of fatal coronary heart disease associated with diabetes in men and women: meta-analysis of 37 prospective cohort studies. BMJ. 2006;332(7533):73-78. doi:10.1136/bmj.38678.389583.7C
3. Della Bona, Roberta et al. “Aspirin in Primary Prevention: Looking for Those Who Enjoy It.” Journal of clinical medicine vol. 13,14 4148. 16 Jul. 2024, doi:10.3390/jcm13144148
4. Pradhan AD, Cook NR, Manson JE, Ridker PM, Buring JE. A randomized trial of low-dose aspirin in the prevention of clinical type 2 diabetes in women. Diabetes Care. 2009;32(1):3-8. doi:10.2337/dc08-1206
5. Cho, Leslie et al. “Summary of Updated Recommendations for Primary Prevention of Cardiovascular Disease in Women: JACC State-of-the-Art Review.” Journal of the American College of Cardiology vol. 75,20 (2020): 2602-2618. doi:10.1016/j.jacc.2020.03.060
6. Handelsman, Yehuda et al. “DCRM 2.0: Multispecialty practice recommendations for the management of diabetes, cardiorenal, and metabolic diseases.” Metabolism: clinical and experimental vol. 159 (2024): 155931. doi:10.1016/j.metabol.2024.155931
Powered by WPeMatico

China: The study published in Diabetes Pathophysiology and Complications revealed that impaired thyroid hormone sensitivity was significantly associated with an increased risk of diabetic nephropathy (DN) in euthyroid individuals with type 2 diabetes.
“Higher values of thyroid feedback indices—PTFQI (OR 1.51), TFQI (OR 1.54), and TSHI—along with a lower FT3/FT4 ratio, were linked to greater DN risk,” the researchers reported. “These hormonal alterations corresponded with elevated urinary albumin-to-creatinine ratio (UACR) and reduced estimated glomerular filtration rate (eGFR), indicating worsening kidney function.”
Diabetes affects over 500 million people worldwide, with type 2 diabetes making up over 90% of cases. Diabetic nephropathy is a serious complication, often leading to kidney failure. Early signs are subtle, delaying diagnosis. While thyroid function is linked to DN, single hormone levels may not give the full picture—composite indices assessing thyroid hormone sensitivity may offer better insight into DN risk and progression.
Against the above background, Dengrong Ma, The First Clinical Medical College, Lanzhou University, Lanzhou, Gansu Province, People’s Republic of China, and colleagues aimed to explore the link between reduced thyroid hormone sensitivity and diabetic nephropathy in euthyroid individuals with type 2 diabetes mellitus (T2DM).
For this purpose, the researchers selected 1,305 euthyroid patients with T2DM who were hospitalized at the Endocrinology Department of the First Hospital of Lanzhou University between July 2021 and August 2023. Thyroid hormone sensitivity was assessed using several indices, including PTFQI, TFQI, TSHI, FT3/FT4 ratio, and TT4RI. Patients were divided into four groups based on the quartile levels of these indices. The association between thyroid hormone sensitivity and diabetic nephropathy (DN) was evaluated using binary logistic regression and restricted cubic spline (RCS) analysis.
The study revealed the following findings:
In euthyroid patients with type 2 diabetes, impaired thyroid hormone sensitivity was found to be associated with diabetic nephropathy (DN), elevated UACR, and reduced eGFR. According to the authors, thyroid hormone sensitivity indices provide a more comprehensive evaluation of thyroid function than individual markers like TSH, FT3, or FT4.
The findings emphasize the importance of assessing thyroid hormone sensitivity in T2DM patients for the early detection and management of DN, even when conventional thyroid function tests are within normal ranges. The authors suggest that further research is warranted to better understand the mechanisms linking impaired thyroid hormone sensitivity with DN.
Reference:
Ma, D., Zhao, P., Gao, J., Guo, X., Han, M., Zan, X., … Liu, J. (2025). The Correlation Between Impaired Thyroid Hormone Sensitivity and Diabetic Nephropathy in Euthyroid Patients with Type 2 Diabetes Mellitus. Diabetes, Metabolic Syndrome and Obesity, 18, 1207–1221. https://doi.org/10.2147/DMSO.S507750
Powered by WPeMatico