
Rare Case of Renal Malakoplakia: Nephromegaly and Sepsis After E. coli UTI in Young Healthy Patient
USA: In a rare and complex medical case, a patient developed malakoplakia as a complication of an E. coli urinary tract infection (UTI), highlighting the intricate relationship between bacterial infections and unusual inflammatory responses. This case, recently documented in BMC Nephrology, highlights the need for increased awareness among healthcare providers regarding atypical presentations of UTIs.
“Renal malakoplakia should be considered in patients presenting with nephromegaly and urinary tract infections that do not improve with appropriate antibiotic treatment,” the researchers wrote. “This condition can occur in individuals without identifiable risk factors, as demonstrated by our patient, who underwent whole exome sequencing revealing no reportable variants associated with primary immunodeficiency or other underlying conditions.”
Malakoplakia is an uncommon inflammatory disorder thought to arise from impaired macrophage phagocytic function, leading to a granulomatous reaction. It can manifest in the genitourinary, gastrointestinal, or cutaneous systems, typically in immunocompromised individuals, though it can also occur in immunocompetent patients on rare occasions.
Ayotola Fatola, Department of Medicine, Johns Hopkins University, Baltimore, MD, USA, and colleagues aimed to highlight malakoplakia as showcased in a young immunocompetent patient, discussed the pathological findings indicative of malakoplakia and reviewed available therapies.
The research team described a case of renal malakoplakia in a young, otherwise healthy patient who presented with nephromegaly and sepsis following an E. coli UTI. The discussion focused on the diagnosis and management strategies, including antibiotic selection and the decision to proceed with nephrectomy.
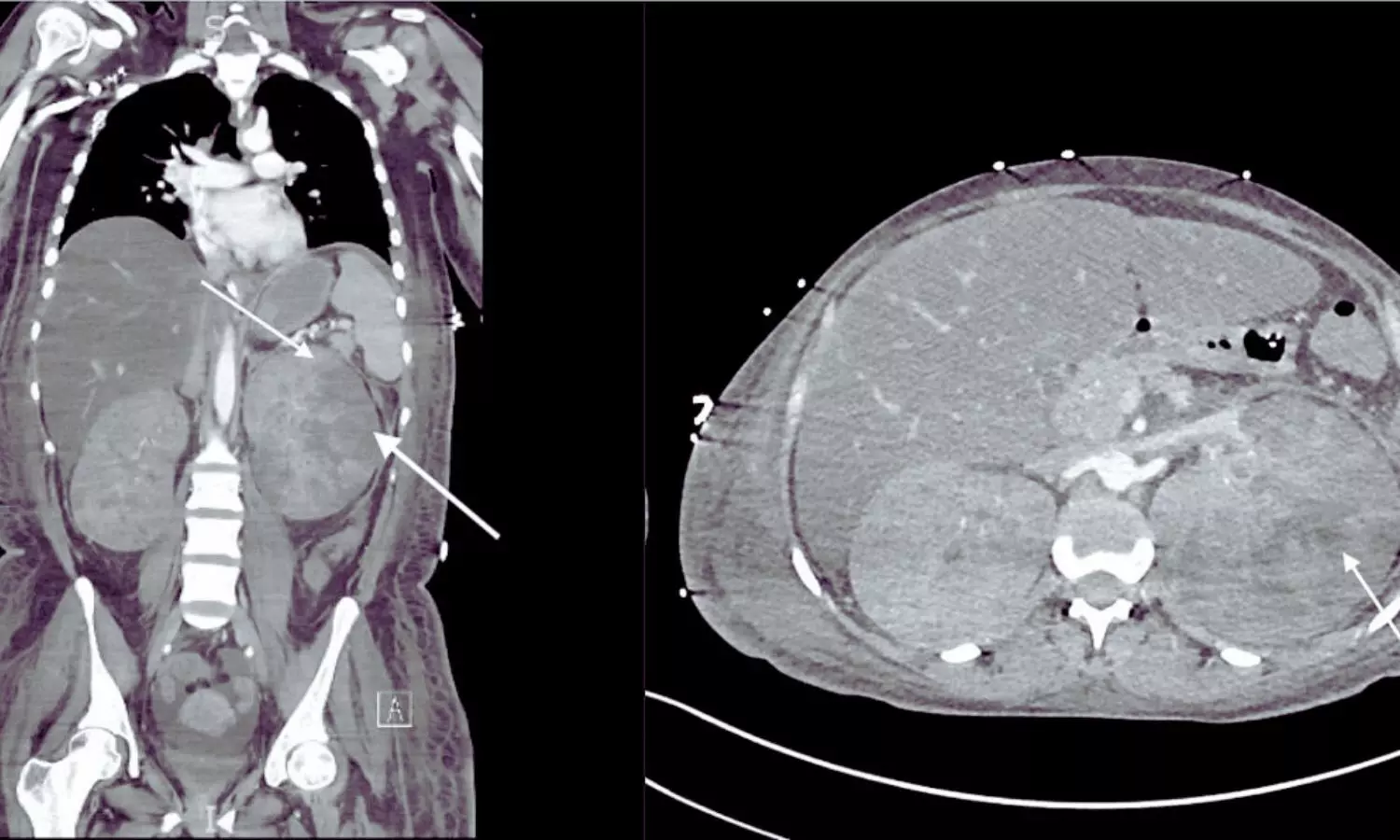
A 32-year-old woman with a history of recurrent UTIs and Raynaud’s phenomenon presented with lower extremity weakness and dyspnea after experiencing UTI-like symptoms a week prior. On admission, she was hypotensive (BP 62/38 mmHg) and exhibited abdominal hepatomegaly and nephromegaly. Neurologically, she displayed 4/5 strength in her lower extremities and absent reflexes, alongside signs of altered mental status. Lab results showed leukocytosis, anemia, thrombocytopenia, and elevated creatinine (6.4 mg/dL). Cultures confirmed E. coli infection.
Imaging revealed massive bilateral kidney enlargement without stones and concern for renal vein thrombosis. Despite broad-spectrum antibiotics, her condition deteriorated, necessitating intubation and continuous venovenous hemodialysis.
A kidney biopsy indicated pyelonephritis with micro-abscesses and histiocytic infiltration, confirming renal malakoplakia. Treatment was adjusted to include tigecycline and aztreonam due to antibiotic resistance, along with ascorbic acid and bethanechol enhancing lysosomal function.
After treatment, her hemodynamics improved, and dialysis was discontinued after 31 days. However, she developed enlarging renal abscesses, leading to a radical left nephrectomy on day 82. Following surgery, her leukocytosis resolved, and she was discharged after 89 days. Three months post-discharge, her kidney function improved significantly, and she continued a 12-month course of oral therapy.
The case underscores the possibility of kidney recovery through extended antibiotic treatment combined with adjunct immunomodulatory therapies and effective source control.
“The optimal management of severe renal malakoplakia is still unclear. This case may provide valuable insights for diagnosis, antibiotic selection, adjunctive therapies, and criteria for considering radical nephrectomy,” the researchers concluded.
Reference:
Fatola, A., Johnson, B.C., Walsh, L. et al. A very complicated UTI: malakoplakia following E. coli urinary tract infection. BMC Nephrol 25, 200 (2024). https://doi.org/10.1186/s12882-024-03640-9

