Revascularization enhances quality of life for patients with chronic limb threatening ischemia: NEJM
Researchers have found in a new study that revascularization may restores sufficient blood flow back into the legs and significantly improves quality of life among patients with chronic limb-threatening ischemia. The study has been published in the New England Journal of Medicine (NEJM).
Over 200 million people around the world are suffering from fever peripheral artery disease (PAD) which is a condition caused by the narrowing of the blood vessels from the heart to the lower limbs.It leads to pain when walking – and for roughly 1-in-10 this advances to chronic limb-threatening ischemia (CLTI).
Those with CLTI often suffer severe pain even at rest, caused by fatty plaque buildup obstructing blood flow, typically to the leg or foot. Those with CLTI face elevated risks of amputation, cardiovascular disease and premature death, yet research on the condition’s impact on quality of life remains limited.
Investigators from both of Mass General Brigham’s founding members, Brigham and Women’s Hospital (BWH) and Massachusetts General Hospital (MGH), as well as Boston Medical Center (BMC), sought to address this problem. Following their previous study highlighting the clinical results of the BEST-CLI trial — Best Endovascular versus Best Surgical Therapy for Patients with Critical Limb Ischemia, the team assessed patient health-related quality of life before and after revascularization treatment. Results are published in Circulation.
“Our study indicates that patients with CLTI have a notably poor quality of life — substantially lower than with many other chronic conditions,” said Matthew Menard, MD, co-director of the Endovascular Surgery Program at BWH and co-principal investigator of BEST-CLI. “Our findings show that revascularization, which restores sufficient blood flow back into the legs, significantly improves quality of life. This confirms the critical role that revascularization plays not just in extending the length of patients’ lives but also its importance in optimizing their wellbeing.”
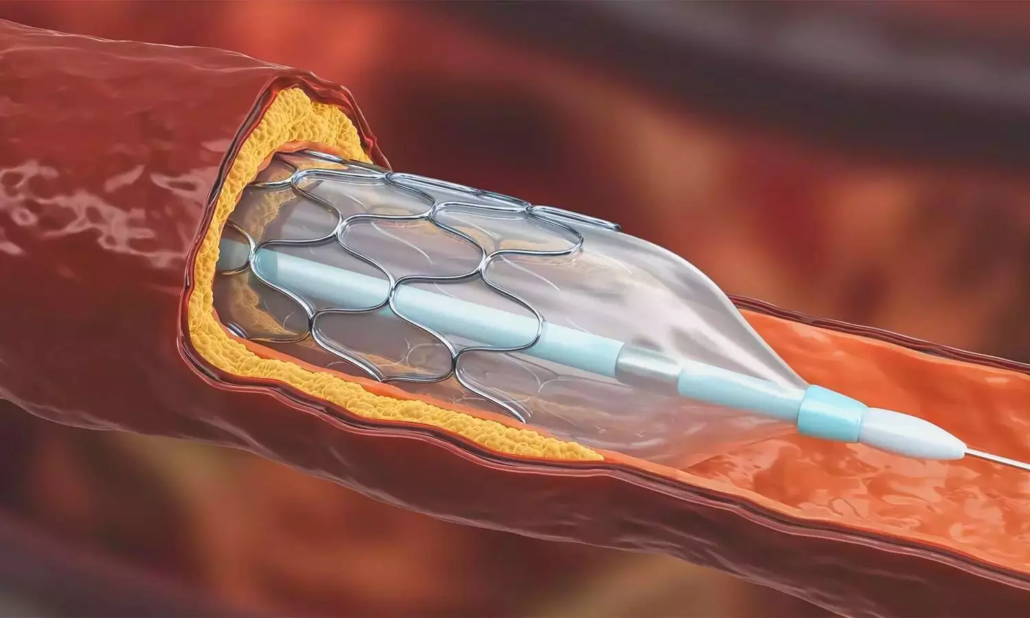
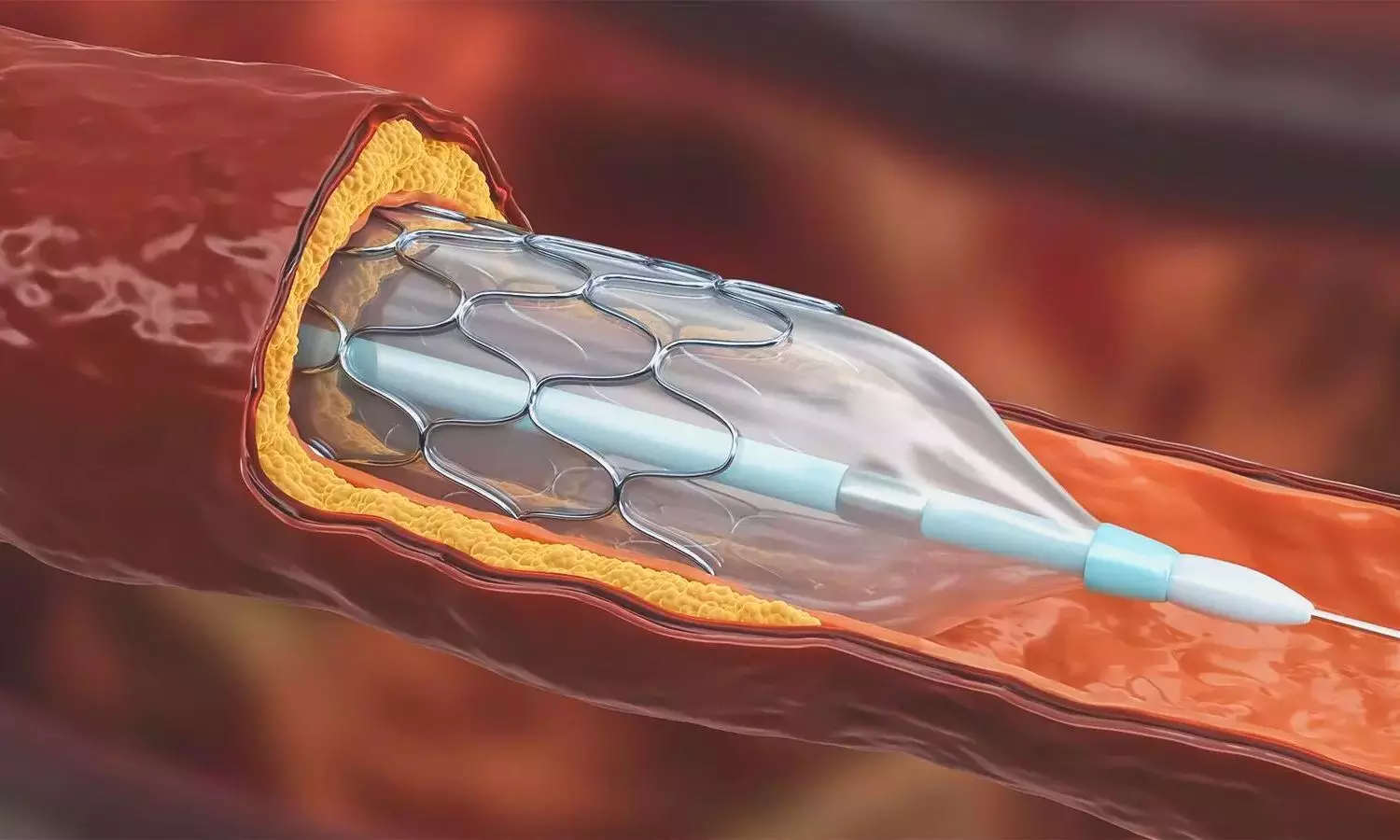
Among patients with CLTI, those eligible for surgical treatment often have two options: surgical bypass (Bypass), where surgeons restore blood and oxygen to the lower limb by reconstructing the blocked vessel, or endovascular therapy (Endo), which involves placing a stent or catheter inside an artery and opening it up to bring blood flow through a blockage.
Funded by the National Heart, Lung, and Blood Institute, with ongoing post-enrollment support from theNovo Nordisk Foundation, the BEST-CLI trial enrolled over 1,800 patients with CLTI from 150 research sites in the U.S., Canada, Finland, Italy, and New Zealand between August of 2014 and October of 2019. Investigators assessed how clinical outcomes (previously reported in NEJM) and quality of life metrics varied between revascularization techniques.
“Medicine is generally moving towards a more patient-centric model of care. That means looking at what’s best for each patient, taking into account an evidence-based approach. Quality of life is one important element in this determination,” said co-principal investigator Kenneth Rosenfield, MD, head of the Section of Vascular Medicine and Intervention in the Division of Cardiology at MGH.
Investigators sorted 1,528 participants into two cohorts. The first cohort was made up of 1,193 patients, all of whom had an available, good-quality, single-segment great saphenous vein (SSGSV), which previous studies have shown is optimal for Bypass. The second cohort was made up of 335 patients who did not have an available SSGSV. Patients in both cohorts were randomized to undergo Bypass or Endo procedures. Researchers assessed quality of life by administering voluntary surveys asking participants about pain levels, activities of daily living, disease symptoms and severity, physical activity, and mental health (anxiety and depression). Surveys were collected at baseline, 30 days post-procedure, at three months, 12 months, then once yearly until the end of the study.
“Patient-reported outcome measures are essential to our understanding of the patient experience,” said co-principal investigator Alik Farber, MD, MBA, interim chair of the Department of Surgery, chief of the Division of Vascular and Endovascular Surgery at BMC and professor of Surgery and Radiology at Boston University Chobanian & Avedisian School of Medicine. “Yet these metrics are not often used and sometimes ignored. Here we found an opportunity to hear our patients’ voices and use them to improve CLTI outcomes.”
While the trial’s previously published clinical outcomes revealed that patients treated with Bypass had fewer major amputations and less need for repeat procedures than those treated with Endo, quality of life did not significantly differ between treatments. Survey results instead revealed that participants generally experienced significant improvements in quality of life after treatment, regardless of their cohort or whether they underwent Bypass or Endo. They further highlighted that patients with CLTI overwhelmingly conveyed that their quality of life was low upon entering the trial, before receiving treatment.
This study is limited in that patients filled out quality-of-life questionnaires at distinct periods throughout the trial, but these time points did not necessarily line up with significant health events such as additional revascularization procedures or amputations. Further, there remains a dearth of quality-of-life research for patients with PAD, and there are no specific metrics to assess the quality of life for patients with PAD or CLTI.
Going forward, the team aims to assess differences in the cost-effectiveness of these procedures, and how cost, among other factors, affects patient quality of life and overall health outcomes.
“The next step is to integrate quality-of-life measures into a more sophisticated care plan to account for the clinical status of the patient and the cost-effectiveness of treatment options, both for the patient and the viability of the healthcare system,” said Farber.
Reference: Matthew T. Menard, Alik Farber, Richard J. Powell, Kenneth Rosenfield, Michael S. Conte, Taye H. Hamza, John A. Kaufman, Mark J. Cziraky, Mark A. Creager, Michael D. Dake, Michael R. Jaff, Diane Reid, George Sopko, Christopher J. White, Michael B. Strong, Max van Over, Emiliano Chisci, Philip P. Goodney, Bruce Gray, Ahmed Kayssi, Jeffrey J. Siracuse and Niteesh K. Choudhry and for the BEST-CLI Investigators Originally published10 Apr 2024https://doi.org/10.1161/CIRCULATIONAHA.123.065277Circulation. 2024;0

